part of Funding The Frontlines: A Roadmap To Supporting Health Equity Through Abortion Access
Home: The Need to Shift Funding to Local Providers
When funders prioritize abortion access in their communities, they are investing in the collective care of the entire area.
According to the U.S. Census, nearly 38% of those who classify themselves as women[*] aged 15-44 lived in one of the 89% of U.S. counties with no clinics providing abortion care. [i] The majority, or 62%, of those seeking abortion care identify as Black, Hispanic, Asian, or Pacific Islanders.[ii]

Click here for more data graphics
The limiting of services and denial of care creates additional hurdles for personal and community success. Three-fourths of abortion patients are low income and less likely to have the resources to navigate through additional barriers to access.[iii] Changes like the closing of a local abortion clinic can have cascading ripple effects – like having to traveling longer distances, less pay due to having to request more time off work, more costs such as overnight lodging and transportation – that can lead to delayed care and result in more costly procedures.[iv]
People who are denied access to health care are likely to experience perpetual economic hardships compared to those able to receive their abortions. It is 4 times as likely that the mother and child will live below the federal poverty line.[v] A 2018 study estimated that women* denied abortions are less likely to be employed full-time and more likely to receive public assistance in the 4 years following the denial.[vi]
By ignoring the financial and physical access to abortion services, funders miss an opportunity to ensure the physical, social, and economic wellbeing of communities they care about.
ENDNOTES
*Data pulled and referenced from the U.S. Census uses self-identified gender categories.
i Jones RK, Witwer E and Jerman J, Abortion Incidence and Service Availability in the United States, 2017, New York: Guttmacher Institute, 2019, https://www.guttmacher.org/report/abortion-incidence-service-availability-us-2017.
ii Jerman J, Jones RK and Onda T, Characteristics of U.S. Abortion Patients in 2014 and Changes Since 2008, New York: Guttmacher Institute, 2016, https://www.guttmacher.org/report/characteristics-us-abortion-patients-2014.
v Diana Greene Foster, M. Antonia Biggs, Lauren Ralph, Caitlin Gerdts, Sarah Roberts, and M. Maria Glymour, 2018: Socioeconomic Outcomes of Women Who Receive and Women Who Are Denied Wanted Abortions in the United States, American Journal of Public Health 108, 407_413, https://doi.org/10.2105/AJPH.2017.304247.
Like most healthcare, community abortion care is provided in a variety of settings, including hospitals, private doctors’ offices, and independent clinics and advocacy centers. However, it is independent clinics, often locally operated as small businesses, that support most individuals seeking abortion services[vii], committing to an outpatient care model at a low cost.
Of the 1,537 facilities nationally that provide abortion services, only 337 – or 21% — are independent clinics. However, these clinics provide the vast majority of care (58% of all services in 2020). This may surprise people who assume that a national group such as Planned Parenthood is the primary provider of abortion care – in fact of the almost 600 PPFA health clinics nationwide, less than half (48%) provide in-person and medication abortion services.[viii]
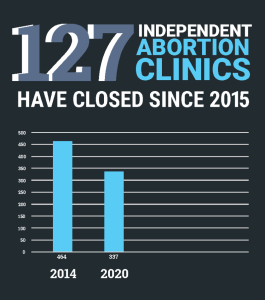 The feminist leaders and physicians that established these independent facilities curated them to provide meaningful, time-sensitive access and intentional care. However, rising costs, shrinking revenues, and increased political pressure and legal restrictions are causing many independent centers to either limit operations or shut down altogether. Since 2015, 127 independent clinics – or 27 percent – have ceased operations.[ix] From 2019-2020 alone, 41 independent clinics have closed in the United States, and 76% of those clinics provided care after the first trimester.[x]
The feminist leaders and physicians that established these independent facilities curated them to provide meaningful, time-sensitive access and intentional care. However, rising costs, shrinking revenues, and increased political pressure and legal restrictions are causing many independent centers to either limit operations or shut down altogether. Since 2015, 127 independent clinics – or 27 percent – have ceased operations.[ix] From 2019-2020 alone, 41 independent clinics have closed in the United States, and 76% of those clinics provided care after the first trimester.[x]
Traditionally, funding local independent community access providers is often an afterthought for philanthropy– the top 20 recipients of reproductive rights funding are national organizations.[xi] With philanthropy on the sidelines, national fundraising efforts, like the Abortion Care Network’s Keep Our Clinics campaign, are left to address this crisis of support and shortage of care options.
vii Jones RK, Witwer E and Jerman J, Abortion Incidence and Service Availability in the United States, 2017, New York: Guttmacher Institute, 2019 https://www.guttmacher.org/report/abortion-incidence-service-availability-us-2017.
viii Abortion Care Network, Communities Need Clinics: The Essential Role of Independent Abortion Clinics in the United States”, December 2020. https://abortioncarenetwork.org/wp-content/uploads/2020/12/CommunitiesNeedClinics-2020.pdf.
xi NCRP analysis of Candid data using the “reproductive rights” subject code. “Reproductive justice” is not a code that exists in Candid.
Roughly a third of U.S. independent abortion clinics belong to the Abortion Care Network (ACN) and its experience supporting access provides key insights to challenges facing providers.

In total, the 22 clinics that had philanthropic funding data available received approximately $15 million total between 2015-2018 from foundations. That is an average of less than $200,000 per year per clinic. In 2020, the ACN campaign Keep Our Clinics also raised and distributed $250,000 from individual donors to clinics[xii]; however it was only a fraction of the $1.4 million requested by their clinic members for clinic supplies, maintenance, and security.[xiii]
The remaining clinics in the network operate as small businesses without the institutional recognition and backing of large health systems and hospitals. These facilities, which represent nearly 80% of all independent clinics, rely primarily on individual donors and service fees. There are only 16 states where clinics are eligible for state funding for abortion services.[xiv]
ENDNOTES
xiiAbortion Care Network, Communities Need Clinics: The Essential Role of Independent Abortion Clinics in the United States, December,2020 https://abortioncarenetwork.org/wp-content/uploads/2020/12/CommunitiesNeedClinics-2020.pdf
xiiiNCRP analysis of Candid data.
xiv Guttmacher Institute, State Funding of Abortion Under Medicaid, July 2021.https://www.guttmacher.org/state-policy/explore/state-funding-abortion-under-medicaid
The COVID-19 pandemic was just the latest challenge threatening the existence of clinics. Debilitating COVID-related expenses included increased costs to comply with social distancing, additional purchases of personal protective equipment (PPE) and greater cost and complication of coordinating travel for doctors and patients.
Equitable staffing is also constant challenge.[xv] In comparison to other medical professions, the reproductive access field is under-staffed with high demand.[xvi] Less than a quarter of the 42,720 OBGYNs nationwide performed abortions in 2019.[xvii] Nationally there are 1700 known providers, including hospitals and doctor’s offices, though many doctors travel across state lines to provide abortion care in more hostile states.[xviii]
 In cases where staff travel from other areas, clinic owners must allocate much of their budgets to not only pay the providers, but to cover travel costs and necessary security improvements as clinic staff experience constant threats.[xix] In addition to their physical safety, clinic owners must find space in their budgets to support staffs’ legal fees when their jobs are being threatened by the state. [xx]In addition to their physical safety, clinic owners must find space in their budgets to support staffs’ legal fees when their jobs are being threatened by the state.
In cases where staff travel from other areas, clinic owners must allocate much of their budgets to not only pay the providers, but to cover travel costs and necessary security improvements as clinic staff experience constant threats.[xix] In addition to their physical safety, clinic owners must find space in their budgets to support staffs’ legal fees when their jobs are being threatened by the state. [xx]In addition to their physical safety, clinic owners must find space in their budgets to support staffs’ legal fees when their jobs are being threatened by the state.
These challenges are on top of an increasingly antagonistic relationship between local government, state legislatures and reproductive access advocates. The first five months of 2021 alone saw six-week abortion bans signed into law in Texas, Idaho, Oklahoma.[xxi] Targeted Regulation of Abortion Providers (TRAP) laws in 23 states require costly licenses to operate and adding new restrictions on where clinics can be located. [xxii]Restrictions on public and private insurance coverage also threaten to increase out-of-pocket costs for patients who are already cash-strapped. All these legal and administrative responses increase the likelihood of that more people will be denied care and create greater pressure for clinics to close or limit abortion services.[xxiii]
As these local efforts tighten options for providers, philanthropy’s response has virtually muted the voice of independent clinics, further jeopardizing their existence. The sector’s emphasis on protecting the legal framework around Roe vs. Wade has led to funding that overwhelmingly flows to policy advocates and lawyers at large national reproductive rights organizations with very little grassroots accountability. This imbalance has made it difficult not just to build community-based power against these policies, but also to meet the urgent need for on-the-ground practitioners and services now.
ENDNOTES
xv It should be noted that there is little data regarding how many doctors are providing abortions in any setting as many do not feel safe enough to be transparent and disclose that they hold this work. Providers are also scarce as a result of the lack of training, willingness and policies that limit provider autonomy.
xvi Association of American Medical CollegesActive Physicians in the Largest Specialties, 2019 https://www.aamc.org/data-reports/workforce/interactive-data/active-physicians-largest-specialties-2019.
xviiMelissa Healy, “OB-GYNs remain conflicted about abortion, survey shows, but pills may be changing attitudes,”Los Angeles Times, February 8, 2019, https://www.latimes.com/science/sciencenow/la-sci-sn-doctors-medical-abortion-20190208-story.html
xviiiSoumya Karlamangla, “60 hours, 50 abortions: A California doctor’s monthly commute to a Texas clinic,” Los Angeles Times, February 8, 2019 , https://www.latimes.com/local/great-reads/la-me-col1-abortion-doctor-20190124-htmlstory.html
xx National Abortion Federation, 2019 Violence and Disruption Statistics, https://5aa1b2xfmfh2e2mk03kk8rsx-wpengine.netdna-ssl.com/wp-content/uploads/NAF-2019-Violence-and-Disruption-Stats-Final.pdf.
xxi Elizabeth Nash and Lauren Cross, Guttmacher Institute, 2021 Is on Track to Become the Most Devastating Antiabortion State Legislative Session in Decades, April 2021 https://www.guttmacher.org/article/2021/04/2021-track-become-most-devastating-antiabortion-state-legislative-session-decades.
xxii Guttmacher Institute, Targeted Regulation of Abortion Providers, July 2021 https://www.guttmacher.org/article/2021/04/2021-track-become-most-devastating-antiabortion-state-legislative-session-decades.
xxiii Elizabeth Nash and Lauren Cross, Guttmacher Institute, 2021 Is on Track to Become the Most Devastating Antiabortion State Legislative Session in Decades, April 2021 https://www.guttmacher.org/article/2021/04/2021-track-become-most-devastating-antiabortion-state-legislative-session-decades.
Since 2020, the Keep Our Clinics campaign has enabled the Abortion Care Network to support clinics, but the need dwarfs the funds, especially in the face of increasing state and federal restrictions. Through the campaign, ACN distributed $250,000 to clinics to support increased expenses in 2020, but 57% of clinics reported that they anticipated a financial loss of at least $25,000 per month due to Covid-19.[xxiv]

Leading foundations, such as The David and Lucile Packard Foundation and Tara Health Foundation, have responded by supporting independent clinics that operate as small businesses indirectly by supporting the Abortion Care Network. Since so many independent clinics are not 501c3 organizations, a grantmaking strategy that focuses on organizations like ACN or supports similar small businesses service providers is one that others in the sector could certainly follow.
Abortion Care Network, Communities Need Clinics: The Essential Role of Independent Abortion Clinics in the United States, December,2020 https://abortioncarenetwork.org/wp-content/uploads/2020/12/CommunitiesNeedClinics-2020.pdf
Over the past several decades, medical professionals and policymakers have come to recognize that the best healthcare solutions are those that are funded at every intersection. It’s time that abortion be invited into those portfolios. There is an urgent and necessary opportunity for independent clinics and providers to exist in grants that center health equity, economic justice, entrepreneurship, or maternal mortality.
It is time for healthcare and women’s foundations to actively join those behind the doors of independent clinics that tend to waiting areas, front desk, exam rooms and labs in the local fight for patient access and safety. It is time to visibly include providers in clinic settings, not just policy wonks, in philanthropy’s definition of abortion access and advocacy. Organizers along the frontline must be seen and funded for movements to thrive and for reproductive liberation to be achieved.
*Data pulled and referenced from the U.S. Census uses self-identified gender categories.
i Jones RK, Witwer E and Jerman J, Abortion Incidence and Service Availability in the United States, 2017, New York: Guttmacher Institute, 2019, https://www.guttmacher.org/report/abortion-incidence-service-availability-us-2017.
ii Jerman J, Jones RK and Onda T, Characteristics of U.S. Abortion Patients in 2014 and Changes Since 2008, New York: Guttmacher Institute, 2016, https://www.guttmacher.org/report/characteristics-us-abortion-patients-2014.
v Diana Greene Foster, M. Antonia Biggs, Lauren Ralph, Caitlin Gerdts, Sarah Roberts, and M. Maria Glymour, 2018: Socioeconomic Outcomes of Women Who Receive and Women Who Are Denied Wanted Abortions in the United States, American Journal of Public Health 108, 407_413, https://doi.org/10.2105/AJPH.2017.304247.
vii Jones RK, Witwer E and Jerman J, Abortion Incidence and Service Availability in the United States, 2017, New York: Guttmacher Institute, 2019 https://www.guttmacher.org/report/abortion-incidence-service-availability-us-2017.
viii Abortion Care Network, Communities Need Clinics: The Essential Role of Independent Abortion Clinics in the United States”, December 2020. https://abortioncarenetwork.org/wp-content/uploads/2020/12/CommunitiesNeedClinics-2020.pdf.
xi NCRP analysis of Candid data using the “reproductive rights” subject code. “Reproductive justice” is not a code that exists in Candid.
xiiAbortion Care Network, Communities Need Clinics: The Essential Role of Independent Abortion Clinics in the United States, December,2020 https://abortioncarenetwork.org/wp-content/uploads/2020/12/CommunitiesNeedClinics-2020.pdf
xiiiNCRP analysis of Candid data.
xiv Guttmacher Institute, State Funding of Abortion Under Medicaid, July 2021.https://www.guttmacher.org/state-policy/explore/state-funding-abortion-under-medicaid
xv It should be noted that there is little data regarding how many doctors are providing abortions in any setting as many do not feel safe enough to be transparent and disclose that they hold this work. Providers are also scarce as a result of the lack of training, willingness and policies that limit provider autonomy.
xvi Association of American Medical CollegesActive Physicians in the Largest Specialties, 2019 https://www.aamc.org/data-reports/workforce/interactive-data/active-physicians-largest-specialties-2019.
xviiMelissa Healy, “OB-GYNs remain conflicted about abortion, survey shows, but pills may be changing attitudes,”Los Angeles Times, February 8, 2019, https://www.latimes.com/science/sciencenow/la-sci-sn-doctors-medical-abortion-20190208-story.html
xviiiSoumya Karlamangla, “60 hours, 50 abortions: A California doctor’s monthly commute to a Texas clinic,” Los Angeles Times, February 8, 2019 , https://www.latimes.com/local/great-reads/la-me-col1-abortion-doctor-20190124-htmlstory.html
xx National Abortion Federation, 2019 Violence and Disruption Statistics, https://5aa1b2xfmfh2e2mk03kk8rsx-wpengine.netdna-ssl.com/wp-content/uploads/NAF-2019-Violence-and-Disruption-Stats-Final.pdf.
xxi Elizabeth Nash and Lauren Cross, Guttmacher Institute, 2021 Is on Track to Become the Most Devastating Antiabortion State Legislative Session in Decades, April 2021 https://www.guttmacher.org/article/2021/04/2021-track-become-most-devastating-antiabortion-state-legislative-session-decades.
xxii Guttmacher Institute, Targeted Regulation of Abortion Providers, July 2021 https://www.guttmacher.org/article/2021/04/2021-track-become-most-devastating-antiabortion-state-legislative-session-decades.
xxiii Elizabeth Nash and Lauren Cross, Guttmacher Institute, 2021 Is on Track to Become the Most Devastating Antiabortion State Legislative Session in Decades, April 2021 https://www.guttmacher.org/article/2021/04/2021-track-become-most-devastating-antiabortion-state-legislative-session-decades.
xxiv Abortion Care Network, Communities Need Clinics: The Essential Role of Independent Abortion Clinics in the United States, December,2020 https://abortioncarenetwork.org/wp-content/uploads/2020/12/CommunitiesNeedClinics-2020.pdf
A convenient way to get the latest news and resources that help grantmakers maximize the impact on equity and justice
Sign me up for ROUNDUP now